Today, whilst I should have been doing any number of other things, I was sucked in the (usually) vacuous sinkhole called Facebook, flicking through my feed for the minor thrill of outrage, feeding my sense of superiority over all those others (who are just like me.) Today was a little different though, because instead of all the negative rants and virtue signalling (neither of which I can I absolve myself of) I saw this (HT Jamie for sharing it.)
I found myself weeping as I watched it.
There are personal reasons for this. Many of the steps that these men were taking, I could have taken too. I could have ended up where they were, but I am a white man, born into a different context. The detail of my own story is not really something that I can talk about, other than to say the person/s whose behaviour led to my trauma had it worse than me in their own childhood.
There are also professional – no that isn’t the right word – philosophical reasons for my interest. I spent a whole career working within a mental health system that pathologised shame and distress. It treated people as if their symptoms were more important than their stories. Really. I do not exaggerate.
At the beginning of my career, we social workers kidded ourselves that we were different. We talked about being person-centred, concerned with need, not fitting people into boxes. We even saw what we were doing as subversive, believing ourselves to be both in and against the State. Because of this, in the early days, we were the patron saints of misfits and lost causes- the people that the system regarded as ‘manipulative’ or to have ‘personality disorders’. People who did not easily fit with fiercely defended diagnostic criterias. The longer I worked though, the more we conformed. Patron saintliness led to unsufferable smugness and anyway,was a luxury we could ultimately not afford. After all, the system works, right? People with mental health problems are cured and sent home to get on with their lives?
Well, no. Not really. Mostly, mental health services are concerned with long term management of life-long conditions. There is relatively low turn over. This in itself creates a huge problem, as in becoming ‘patients’ people enter into a process of loss, which is then replaced by a different set of indentity markers. For rather too many, the stigmatising effect of this transfer of identity can have the effect of further traumatising people who were already managing more than their share.
This takes us straight to the old arguments about nature and nurture. What shapes our psychology, our genes or our experiences? Are emotions just chemicals? The answer to all of this is yes. We are not machines – the chemicals that surge through are both cause and effect – but neither can we pretend that the way we seek to modify increasingly levels of psychopathology is working for us.
Of course, I am not saying that people don’t get better, or that they are not helped by the many and varied science-based interventioned offered to them by mental health services. I am just saying that in many cases, the help on offer is very limited and pre-programmed towards protecting the system from overload and risk. It is also entirely obvious that those who get the most out of the mental health care system (as with all other systems) are those who already might be seen to be winners in life’s lottery- the educated, the wealthy and those who already benefit from networks of resillience.
So let’s step in to the circle.
How do we define the kind of trauma that is being referred to in the prison video above?
Most of us will have heard of the list of Adverse Childhood Experiences that give some kind of indication as to our vulnerability as adults. Some of us will have seen questionnaires like this one.
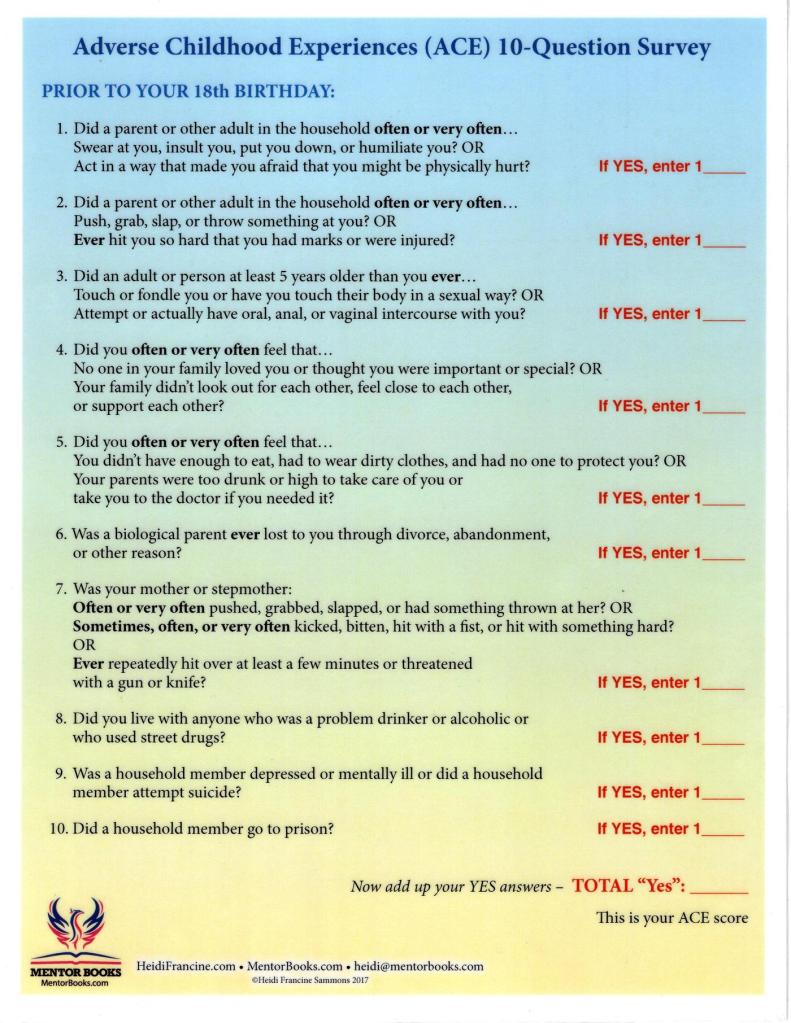
The strange thing about those of us who ahve answered yes to a few of these questions is that we share a secret. Even when we are able to see the fact that we were victimised by the behaviour and problems of someone else, we carry a deep sense of shame. We believe that at some level, it is our own fault. This kind of shame is toxic.
It also brings some rather unique life skills. We are like secret agents in our ability to submerge our feelings. We are also often have a social superpower- not in our ability to manage complex social interactions, but in our ability to read and understand them. Particularly when they involve other kinds of pain and distress.
We ought to be very good at this kind of stuff
But it is easy to fall in to this.
There is only one kryptonite for shame and it is called compassion.
Have a think about that. I don’t mean ‘There there, it’ll be OK’ kind of compassion. I mean the kind that celebrates our shared vulnerbilities. I mean compassion for others, but also (and perhaps even more important) compassion for ourselves.
In the context of our prisons and hospitals (full as they are by people like me) it has to mean something much more visceral and dangerous than what we have seen so far. My friend David sent me a podcast to listen to a couple of years ago and it has nagged at me ever since. Here is an excerpt
Trauma, particularly complex trauma, is not solved by being nice. It can take a lifetime to come to terms with, but it has to start with the right questions.
And it has to start with compassion.